




Room Mock-ups & Their Utilization In The Design Process
From major decisions like placement of fixed elements to minor adjustments of just inches, the room mock-up process often justifies the time and money to produce them, particularly if the room is to be replicated within a facility. Kregg Elsass, AIA, knows others too have experience to back this up.
He shares, "At a recent Healthcare design conference, an architect shared an experience with a hospital client. The project team had developed room mock-up construction documents for several separate planned spaces such as operating, ICU, emergency treatment and patient rooms. The estimate of $100,000 to actually build the room mock-ups was submitted to the owner, who decided to pass instead of allowing the team to identify ways to reduce that cost."
Out of an $80M-plus total construction price tag, the architect explained to his peers even a reduced scope of that $100,000 probably would been the most valuable line item in the client’s budget as the mock-ups would have substantially increased the probability that the rooms ultimately would provide the desired outcome. While the client explained to the project team, “we trust our architects to give us the right design and we feel it is unnecessary to spend this money”, in reality, the issue had nothing to do with trust but instead everything to do with quality design results.
Kregg elaborates, "Outside of the design profession, the cost to construct mock-ups can be perceived as pulling funds away from as opposed to enhancing the value of the design. Mock-ups allow designers to consider broad issues such as placement of walls or assessment of room sizes and proportions, as well as refinement of room details. A matter of only inches can make a difference when positioning an element of a room attribute that elevates the design from simply meeting requirements to ensuring that element is in exactly the right spot to maximize functionality. Since drawings, even computerized 3-D renderings, are a fraction of actual size it is virtually impossible to make precise decisions unless the rooms are full-scale. While architects and designers are trained to understand subtleties in drawings, they can fail at ideal location of attributes. Clinicians are not trained in this process so their ability to help at this point is often impossible."

Driving Cars, Using Buildings Are Not Equal
Kregg says, "I feel the simplest way to explain why design and clinical teams need to utilize the mock-up process is to use an analogy of manufacturing automobiles. Essentially, every car on the road today was developed utilizing the mock-up process. In many ways, a 2010 model ends up being a mock-up for the 2013 version, and so on. Each new design is developed as a mock-up and subsequent prototype long before full-scale production kicks into place. Designers test the mock-up, make improvements and then produce a beta model to make final adjustments prior to mass production. Even with this extensive pre-production activity, consider how many recalls automotive manufacturers have issued to correct mistakes. There are so many variables in the automobile production process and the same is true in the building construction industry.
"However, every building that gets built is a new mock-up. That particular building on that particular site, constructed at that time by that particular contractor, has never been designed and constructed before. Therefore there is little reason to think that it will be free of mistakes or opportunities for improvement. Room mock-ups can go a long way to identifying elements that could be corrected prior to construction."
Room Attributes
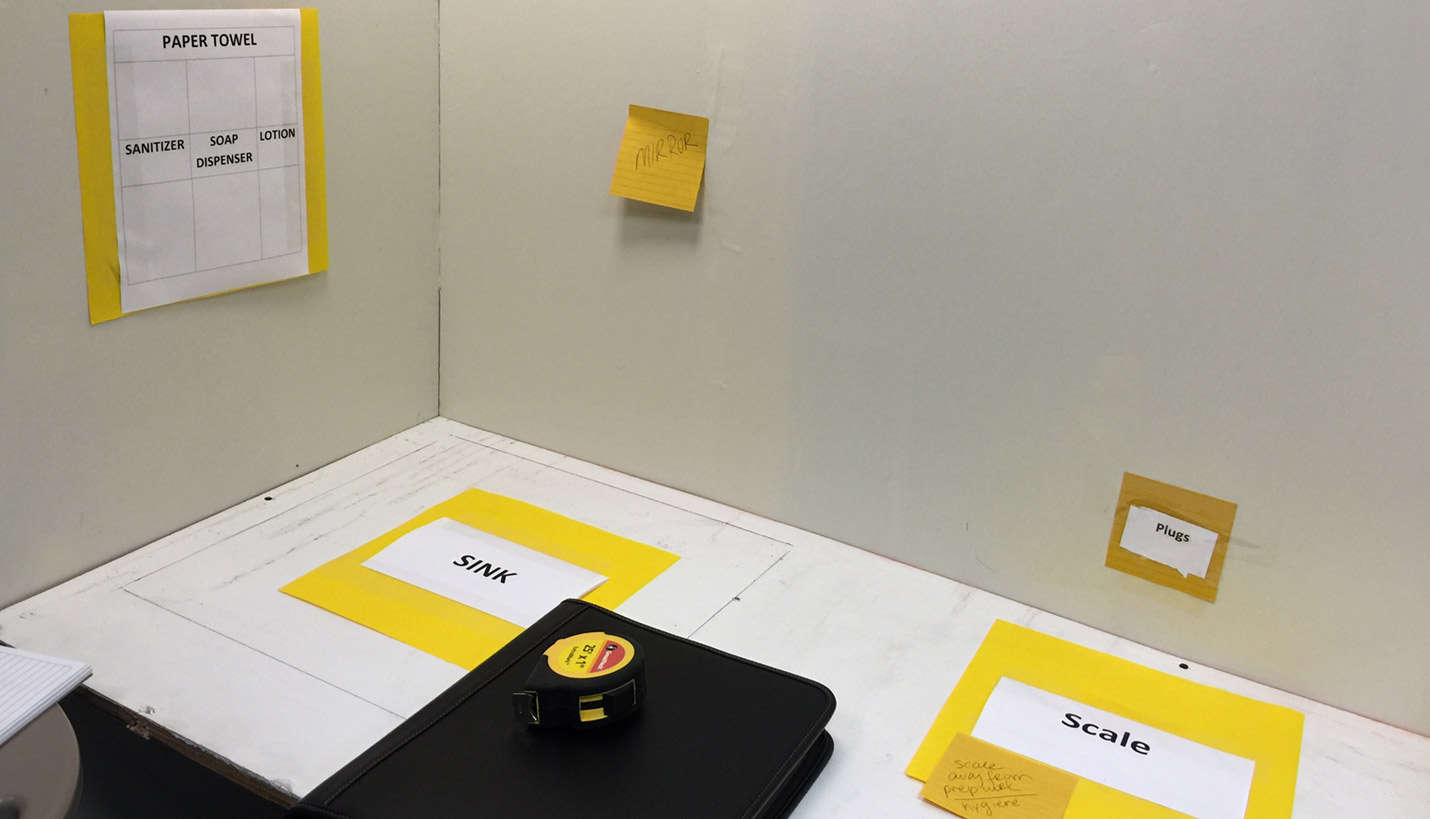
Sometimes the benefits of constructing a mock-up still make sense, even if it is constructed without being identified as an additional service and even if it has to be built in the architect’s own office. If unique ideas and concepts are being developed, it is too risky to simply review shop drawings and hope for the best. In one case, a Page design and planning team came in on a Saturday and found a back corner in the office with sufficient space to build at least one of the rooms they had determined needed to be mocked up.
On another project a Page team was in the process of developing a 36-OR perioperative suite for a large teaching facility. During the preliminary design and subsequent schematic design process, there was substantial input and review from all levels of the institution; administration, facility personnel, surgeons, nurses, directors and staff. The basic organization of the OR suite evolved into the perimeter racetrack concept with internalized sterile work rooms connecting each OR. By the end of the schematic design phase, the structural bays were set and the interior layouts were approved to proceed into design development. After the room mock-up was constructed and toured, the first wave of input from surgeons, nurses and managers was concerning. Even though substantial input had been attained during the process regarding the shape and design of the operating room – including 3-dimensional computer renderings - the initial feedback was that the proportions of the room were problematic and would have to be changed.
Kregg explains, "On this particular project we were fortunate the OR equipment manufacturer brought all the major equipment to the mock-up, including the table, surgical light and anesthesia boom. This cooperation created a win-win situation because it allowed for more realism within the mock-up for user assessment - and allowed the manufacturer to display their system to the client. It wasn’t until the actual equipment was placed in the mocked-up 3D space that the problem was identified – not at any time in the process before.
"Think about this for a second. Thirty-six OR rooms constructed for a major teaching facility would have been built with a flaw this particular client would have found unacceptable. The traditional 2D process had failed us, despite decades of collective expertise among the project team. While we had used a similar proportion on other projects that were ideal for those clients, this particular one had a unique use in mind so the same room would not have been suitable. Although some time was lost in going back to re-plan this part of the project, that cost was inconsequential in the big picture.
Putting It Into Perspective
There are numerous other similar examples throughout our industry that justify the time and expense to construct full-scaled room mock-ups. There are other ways to achieve this goal such as having the contractor fit out a repeating room out of construction sequence for use as the mock-up. However, that is not very flexible relative to construction scheduling. If problems arise that take time to resolve, it could very likely jeopardize the construction critical path. We strongly recommend allocating the time and financial resources on the upfront side of the design schedule so there is sufficient opportunity to continue working on mock-ups to resolve design problems long before contractors are involved. This isn’t rocket science, it’s just good design process. The next time you have a client question this recommendation, calculate the percentage of the cost for the mockup against the total budget, including construction. You may find it's less than one percent, if even that.
12/06/2019




People
Related Posts
- 2400 Nueces Wins Green Award
- Reaching for the Stars - 2400 Nueces Grabs Four
- 2400 Nueces Featured in AEGB Sustainability Case Study
- Complementary Competition
- New Generation of Student Living Connects the University of Texas Campus with Adjoining Community
- Case Study: A Typical Medical / Surgical Patient Room Design Mock-up
- Best in Brick: Baylor Surgical Hospital at Fort Worth